Stunting as One of the Nutritional Problems in Indonesia
According to Law no. 36 of 2009 concerning Health, what is meant by health is a state of health, both physically, mentally, spiritually and socially that allows everyone to live a socially and economically productive life. A person's health level is influenced by several factors including being free from disease or disability, good socioeconomic conditions, good environmental conditions, and good nutritional status. Nutritional status is one of the important factors in achieving an optimal degree of health. (Ministry of Health 2017).
Nutritional problems are basically a reflection of the consumption of nutrients that are not sufficient for the body's needs. Insufficient nutritional intake in the diet, can lead to malnutrition, on the contrary people whose nutritional intake is excessive will suffer from more nutrition. So nutritional status is a picture of an individual as a result of daily nutritional intake. Nutritional status can be known through measuring several parameters, then the results of these measurements are compared with standards or references. (Ministry of Health 2017).
Stunting is a physical growth disorder characterized by a decrease in growth speed and is the impact of nutritional imbalances. According to the World Health Organization (WHO) Child Growth Standard, stunting is based on the index of body length compared to age (PB/U) or height compared to age (TB/U) with a limit (z-score) of less than -2 SD. Childhood stunting is a cost and economic burden. This is because it will increase the risk of child death, adversely affect the child's development and learning capacity, increase the risk of infectious diseases and non-communicable diseases, and decrease productivity and economic ability in adulthood. Reducing stunting in childhood is the first of six goals in the Global Nutrition Targets for 2025 and a key indicator in the second Sustainable Development Goal (SDG) to Achieve Zero Hunger (Wicaksono and Harsanti, 2020)
The problem of stunting is experienced by most children in poor and developing countries including Indonesia. Prevalence in Asia such as India (38.4% 2015), Pakistan (45% 2012), Bangladesh (36.1% , 2014), Malaysia (20.7% 2016 ), Philippines, Thailand (10.5% 2017) and Indonesia (30.8%, 2018) ( Budiastutik and Rahfiluddin, 2020). Based on data from the World Health Organization (WHO) Indonesia is ranked 115th out of 150 countries in the world. From the results of the Indonesian Nutritional Status Survey (SSGI) in 2021, the prevalence of stunting in Indonesia was 24.4%, down by 3.3% from the results of SSGI in 2019 which was 27.7% (Purnamaningrum et al., 2021).
Factors Related to the Incidence of Stunting in Toddlers
A. Energy and Protein Intake
Nutrient intake in toddlers is very important in supporting growth in accordance with the growth chart so that growth faltering does not occur which can cause stunting. In 2017, 43.2% of Indonesia's under-fives experienced an energy deficit and 28.5% experienced a mild deficit. For protein adequacy, 31.9% of toddlers experienced a protein deficit and 14.5% experienced a mild deficit as shown in the figure below (Pusdatin Kemenkes, 2017).
B. Infectious Diseases
Reduction in nutritional status occurs due to insufficient nutritional intake and frequent occurrence of infections. So environmental factors, family circumstances and behaviors that facilitate infection have an effect on the nutritional status of toddlers (Trihono et al, 2015).
The reality is that malnutris and infections often occur together. The two influence each other which eventually leads to a vicious circle. The relationship between malnutrition and infection can be seen in the following figure
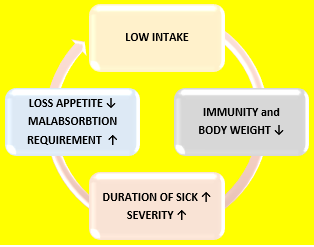
Figure 1. The Relationship between Infection and Malnutrition
C. Exclusive breastfeeding
Breast milk is an important food source for the health of babies. ASI can meet three-quarters of the protein needs of babies aged 6 – 12 months, in addition to breast milk also contains all kinds of essential amino acids needed. Thus, breast milk isanideal form of eating because it is able to meet the nutritional needs of babies in the first six months of life. Exclusive breastfeeding is to give only breast milk to babies from birth to 6 months of age.
Balita who did not get exclusive breastfeeding during the first 6 months were higher in the stunting toddler group (88.2%) compared to the normal toddler group (61.8%). The results of the Chi Square test showed that there was a relationship between exclusive breastfeeding and stunting incidence with an OR of 4,643. (Ni'mah and Nadhiroh, 2015).
From a study conducted by Agustia et al in 2018, it shows that there is a relationship between exclusive breastfeeding and stunting. It can be concluded that toddlers who do not get exclusive breastfeeding have a risk of stunting by 4,659 times higher than toddlers who get exclusive breastfeeding. (Agustia,2018). This result is also in line with that carried out by Rajan et al (2012) and Fikadu et al (2014) in Agustia 2018 which stated that children who did not get exclusive breastfeeding had a risk of stunting of 6.9 times and 3.27 times higher than toddlers who received exclusive breastfeeding (Agustia, 2018).
D. Immunization Status
Immunization isupay a to inflict and increase immunity to diseases in infants. Immunization should be given to infants and toddlers as well as children of primary school age/equivalent. Incomplete immunization causes toddlers to become weak so that it is easy to develop infectious diseases. Children who experience infection if left unchecked can be at risk of stunting (Agustia et al, 2018).
In the study, the results of OR 3.85 were obtained which showed that toddlers who did not get complete basic immunization were at 3.85 times greater risk of stunting compared to toddlers who received complete immunization (Agustia et al, 2018).
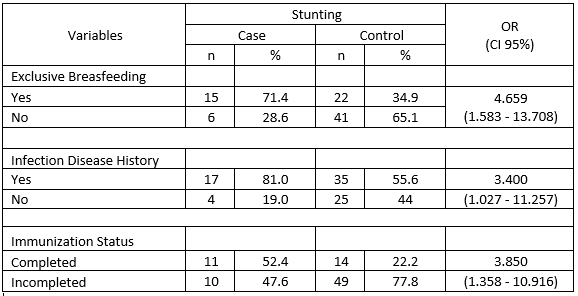 Table 1. Risk Factors for Stunting in Toddlers
Table 1. Risk Factors for Stunting in Toddlers
E. Birth Weight
From a study in the Philippines, toddlers born weighing less than 2,500 grams, had a 3.82 times greater risk compared to toddlers born with normal weight. Furthermore, the risk factor of birth weight less than 2,500 grams has a p value = <0.001. This means that risk factors for birth weight less than 2,500 grams have an influence on the incidence of stunting in toddlers in the Philippines (Apriluana, 2018).
Another study in Indonesia found that toddlers with a birth weight of less than 2,500 grams with hasil statistical tests using logistic regression tests showed p value = 0.047. This means that risk factors for birth weight less than 2,500 grams also have an influence on the incidence of stunting in toddlers in Indonesia (Apriluana, 2018).
F. Birth Length
Based on the research conducted in Kulon Progo that the length of birth in babies if less than 48 cm will be at risk of stunting in the future, based on research in India babies born with small body lengths are at risk of stunting, research in Depok is known that short baby birth lengths are at risk of stunting children in the future, research conducted by Friska et al found that short birth lengths are at risk of 16.4 times stunting (Budihastutik, 2019).
G. Parental Education
Based on research data from Indonesia based on the level of maternal education, namely mothers who did not complete basic education and mothers who completed high school. The results of the logistic regression test showed that the Odds Ratio value for toddlers weighing less than 2,500 grams was 1.67 (95 % CI 1.13-2.47). This means that toddlers with mothers who do not complete primary education have a 1.67 times risk of stunting compared to mothers who complete high school. Furthermore, the risk factor for mothers who did not complete primary education had a p value = <0.001. This means that the risk factors for mothers who do not complete primary education have an influence on the incidence of stunting in toddlers in Indonesia (Apriluana, 2018).
H. Economic Status
Stunting shows the relationship of age dependence among children, especially between the ages of 1-6 years, with inadequate eating or the presence of recurrent diseases or chronic diseases (Apriluana, 2018).
In Riskesdas 2013, the economic status of the population was assessed based on household ownership indicators that had been assessed for validity with the economic status carried out according to Susenas based on the level of household expenditure per capita. The economic status of the population is classified into five namely: i) Quintile 1 – bottom; ii) Quintile 2 – Lower Intermediate; iii) Quintile 3 – Intermediate; iv) Quintile 4 – Upper Intermediate; and v) Quintile 5 – Top. (Riskesdas Report, R&D, 2013) (Trihono dkk, 2015).
Correlation and regression analysis were performed on the population group of quintile 1 and quintile 5 with short nutritional status in toddlers. Plots 1 and 2 are correlations of stunting prevalence in toddlers for quintile 1 and quintile 5, respectively. If the population conditions are with the lowest economic status, it appears that the prevalence of short in toddlers will rise by 0.19 percent with a positive relationship nature. Meanwhile, in the population group with the top economic status, the prevalence of short toddlers will be lower by 0.26 percent with the nature of negatif relations) (Trihono et al, 2015).
G. Parental Education
Based on research data from Indonesia based on the level of maternal education, namely mothers who did not complete basic education and mothers who completed high school. The results of the logistic regression test showed that the Odds Ratio value for toddlers weighing less than 2,500 grams was 1.67 (95 % CI 1.13-2.47). This means that toddlers with mothers who do not complete primary education have a 1.67 times risk of stunting compared to mothers who complete high school. Furthermore, the risk factor for mothers who did not complete primary education had a p value = <0.001. This means that the risk factors for mothers who do not complete primary education have an influence on the incidence of stunting in toddlers in Indonesia (Apriluana, 2018).
H. Economic Status
Stunting shows the relationship of age dependence among children, especially between the ages of 1-6 years, with inadequate eating or the presence of recurrent diseases or chronic diseases (Apriluana, 2018).
In Riskesdas 2013, the economic status of the population was assessed based on household ownership indicators that had been assessed for validity with the economic status carried out according to Susenas based on the level of household expenditure per capita. The economic status of the population is classified into five namely: i) Quintile 1 – bottom; ii) Quintile 2 – Lower Intermediate; iii) Quintile 3 – Intermediate; iv) Quintile 4 – Upper Intermediate; and v) Quintile 5 – Top. (Riskesdas Report, R&D, 2013) (Trihono dkk, 2015).
Correlation and regression analysis were performed on the population group of quintile 1 and quintile 5 with short nutritional status in toddlers. Plots 1 and 2 are correlations of stunting prevalence in toddlers for quintile 1 and quintile 5, respectively. If the population conditions are with the lowest economic status, it appears that the prevalence of short in toddlers will rise by 0.19 percent with a positive relationship nature. Meanwhile, in the population group with the top economic status, the prevalence of short toddlers will be lower by 0.26 percent with the nature of negatif relations) (Trihono et al, 2015).
Conclusion
The problem of stunting is experienced by most children in poor and developing countries including Indonesia. Stunting will increase the risk of child death, adversely affect children's development and learning capacity, increase the risk of infectious diseases and non-communicable diseases, and reduce productivity and economic ability in adulthood.
There are many factors that influence the incidence of stunting in children such as the amount of calorie intake and protein after infection which is the direct cause. In addition, there are also other factors that play a role, namely exclusive breastfeeding, immunization status, education andparental knowledge, economic status, weight and length of birth. Reducing stunting in childhood is the first of six goals in the Global Nutrition Targets for 2025 and a key indicator in the second Sustainable Development Goal (SDG) for Achieve Zero Hunger.
Referrences
- Thamaria, N., 2017, Nutritional Status Assesment, Center for Health Human Resources Education, Indonesia Ministry of Health, Republic of Indonesia
- Wicaksono F. and Harsanti T., 2020, Determinants of Stunted Children in Indonesia : A MultilevelAnalysis at the Individual, Household, and Community Levels, National Public Health Journal
- Purnamaningrum YE., et al, 2021, Analysis of Factor Related To Stunting in Children Aged 2 – 5 Years, Interest : Jurnal Ilmu Kesehatan.
- Centre of Health Data and Information, 2018, Situation of Children with Stunting in Indonesia, Minsitry of Health, Republic of Indoensia, ISSN 2088 – 270 X
- Ni’mah K and Nadiroh SR., Factors Realted to Stunting Event in Toddlers, Media Gizi Indonesia, Vol. 10, No. 1 January – June 2015: page. 13–19
- Agustia R., et al., 2018, Risk Factors Stunting Events at Toddlesrs at 12 – 59 Months in Pobaya Mine Area Palu City, Health and Nutrition Journals
- Apriluana G and Fikawati S., 2018, Analysis of Risk Factors of Stunting Among Children 0-59 Months in Developing Countries and Southeast Asia, Media Litbangkes, Vol. 28 No. 4, Desember 2018, page 247 – 256
- Budiastutik I and Rafihluddin MZ., 2019, Risk Factors of Child Stunting in Developing Countries, Amerta Nutr 122 – 126
- Trihono et al, 2015, Stunting in Indonesia, Its Problems and Solutions, Agency for Health Research and Development, Ministry of Health, Republic of Indonesia
